What is Blood Pressure & How Your Heart Works
Blood pressure is the force exerted by circulating blood on the walls of blood vessels. The heart is a pump, and arteries are pipes. Each heartbeat pushes a volume of blood into the arteries, momentarily increasing the force on the walls. Then, the heart relaxes, and the force decreases. These two numbers—peak pressure and minimum relaxation—are what the monitor measures.
Normal pressure on arteries stays below 120/80 mmHg. When it consistently exceeds 130/80, arteries begin to adapt by thickening and stiffening. This is the beginning of the problem.
Why does the body need pressure at all? Because blood carries oxygen and nutrients to every cell in your body—from the top of your brain to your fingertips. Without sufficient pressure, blood won't reach the highest points. However, excessive pressure breaks the pipes themselves. Balance is life.
Systolic vs. Diastolic: Two Numbers Tell Two Stories
When a doctor writes "120/80," the top number is called the Systolic pressure, and the bottom is the Diastolic. Each tells you about a different phase of the heart's cycle:
Systolic — The Top Number
- Measures the force at the moment the heart contracts.
- Highlights arterial stiffness.
- Most important after age 50.
- Every 10-point increase = double the risk.
Diastolic — The Bottom Number
- Measures the force when the heart relaxes.
- Reflects resistance in small arteries.
- Most important before age 50.
- Isolated elevation is an early sign.
Pulse Pressure: The Silent Indicator After 40
There's a third number, almost forgotten by patients but crucial for doctors: Pulse Pressure, the difference between systolic and diastolic. If your pressure is 140/70, your pulse pressure is 70—which is high.
A normal difference between the two numbers is 30-40 mmHg. When it exceeds 60 after age 50, it indicates that the large arteries have lost elasticity and are stiffening. Recent research in The Lancet 2023 links high pulse pressure to a 40% increased risk of stroke, independent of systolic pressure alone.
If the difference between your two numbers is over 60 and you're over 50, ask your doctor about arterial stiffness, not just the top number.
Saudi Arabia's Numbers in Facts
According to the Ministry of Health (MOH 2022) and the Saudi Heart Association (SHA 2023), the data reveals the reality:
Source: MOH National Risk Factor Survey 2022 · Saudi Heart Association 2023 · WHO EMRO 2024.
A quarter of Saudi adults have high blood pressure. Half of them don't know. And of those who know, less than a third are effectively managed.
Read Your Monitor: Where Are You on the Scale
When you measure your blood pressure at home or the pharmacy, you get two numbers. Enter them into the following tool to see where you stand on the AHA/ACC 2017 updated 2024 scale:
Thresholds per AHA/ACC 2017 updated 2024. Result is for guidance only and does not replace medical consultation. Record readings twice weekly before any decisions.
Your Risk Factors: An 8-Step Self-Assessment
High blood pressure is often silent. However, risk factors can be identified. Check all that apply to you:
What Happens Inside Your Arteries When Pressure Rises
High blood pressure doesn't hurt because arteries lack pain receptors. But it silently works for years, altering the artery's structure from within. Here are four stages that take decades:
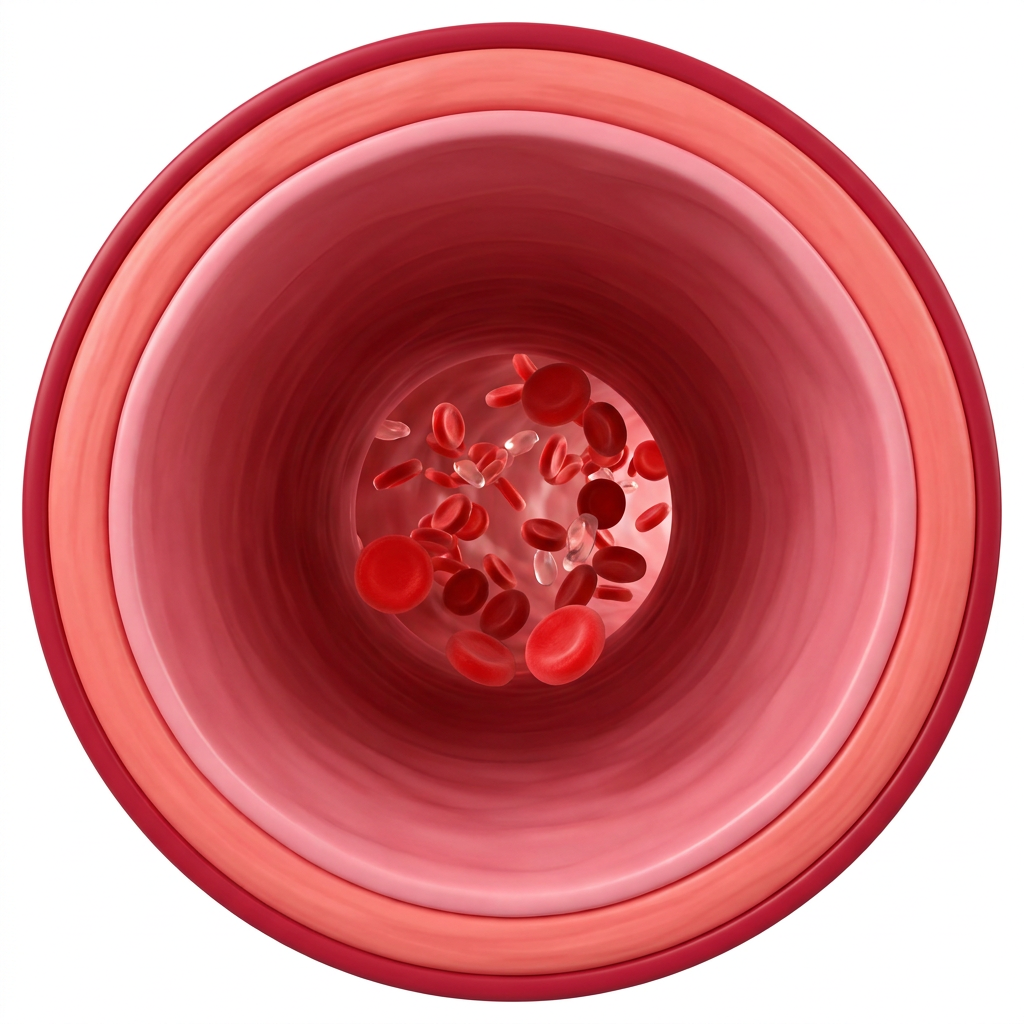
Stage 1 — Flexible Artery
The artery wall is smooth and elastic. With each heartbeat, it expands slightly and returns. Pressure remains normal, and the heart isn't strained.
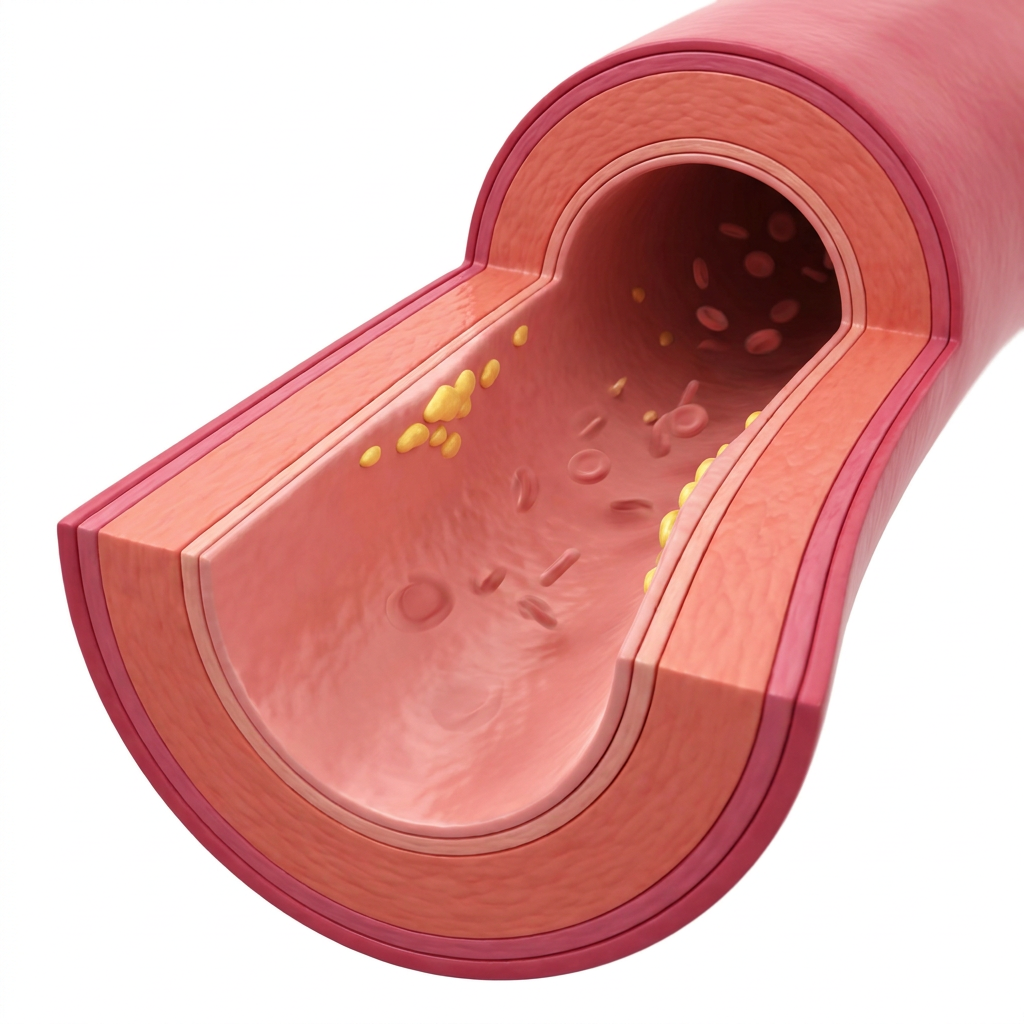
Stage 2 — Early Thickening
The wall begins to thicken as a defensive reaction. The artery loses some elasticity. No symptoms, but the heart works harder to pump blood.
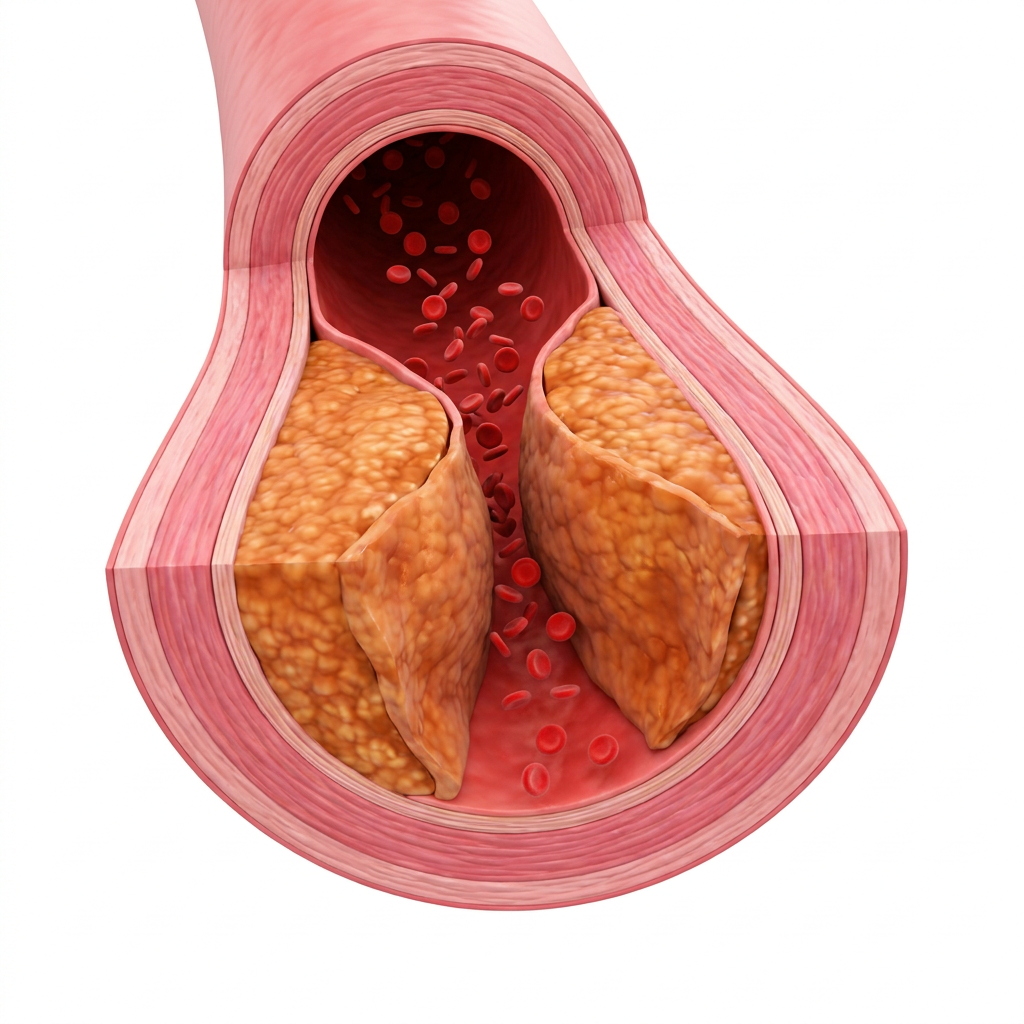
Stage 3 — Stiffening & Narrowing
The wall is rigid, and the lumen is narrow. Pulse pressure increases. Signs appear in the retina and kidneys. The heart enlarges to cope.
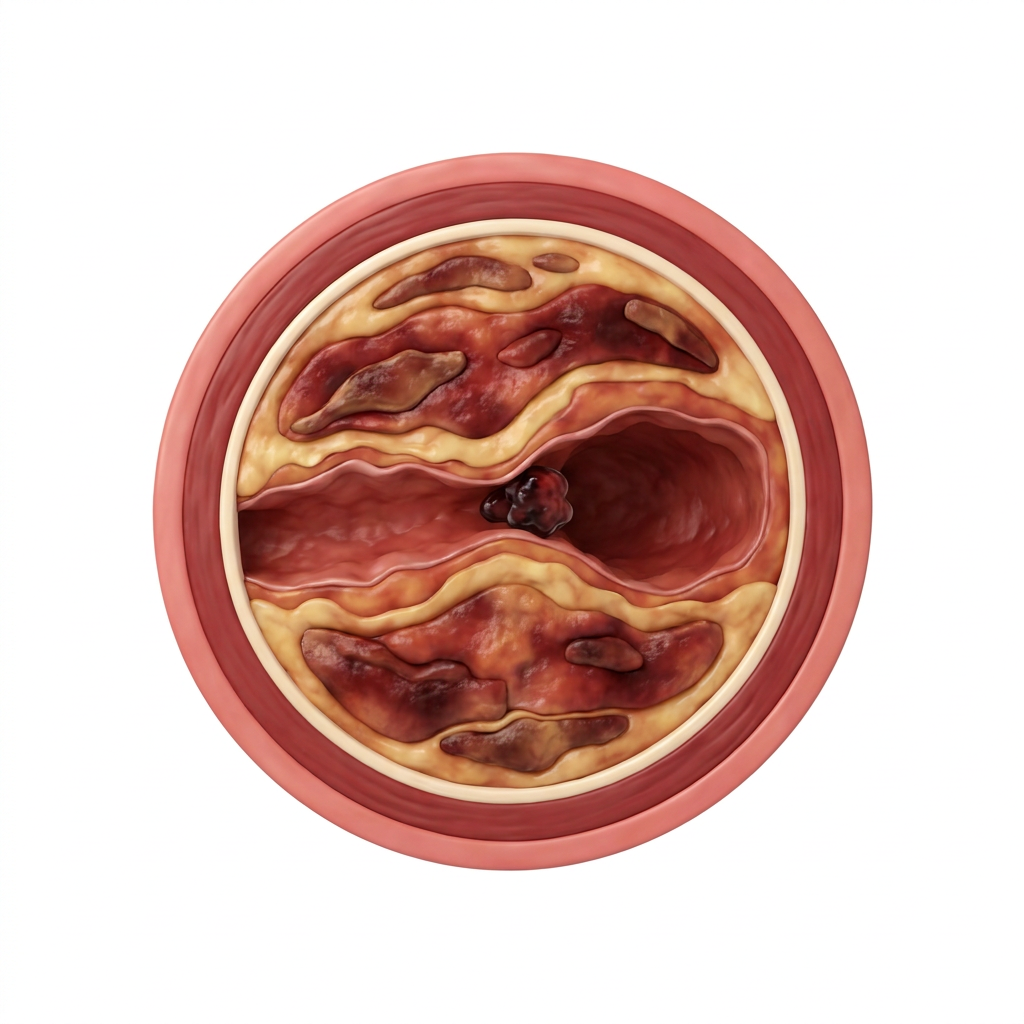
Stage 4 — Organ Damage
Micro-tears in the wall, small clots, kidney failure, heart enlargement, memory impairment. Risk of stroke and heart attack is high.
Your artery adapts with every month under excess pressure. Adaptation isn't a friend—it's a permanent loss of elasticity.
Consequences of Neglect: Stroke, Kidneys, Heart, and Retina
Uncontrolled high blood pressure targets four organs specifically. Any one of them can change your life. All four together are a catastrophe:
Stroke
Chronic hypertension can rupture a delicate brain artery or cause a clot. The result: paralysis, speech loss, or death. 70% of Saudi strokes are due to uncontrolled BP.
Kidney Failure
Kidneys filter blood through tiny capillaries. High blood pressure damages them gradually. Each year of uncontrolled BP costs you 3-5% of kidney function. Dialysis may be the end result.
Heart Failure
The heart strains for years to pump blood through stiff arteries. It enlarges as a response, then weakens. The result: shortness of breath, leg swelling, chronic fatigue. The biggest reason for elderly hospital admissions.
Retinal Damage
The tiny capillaries of the retina are early victims of hypertension. They rupture, bleed, or become blocked. Vision deteriorates gradually. A fundus exam can detect significant hypertension before any other symptom.
Dementia & Alzheimer's
Midlife hypertension, if uncontrolled, doubles the risk of dementia and Alzheimer's after age 60. Tiny brain capillaries are affected early. The SPRINT-MIND 2019 study: Strict BP control reduces cognitive decline risk by about 17%.
Hidden Sodium in Seven Common Sources
The recommended daily sodium intake for hypertensive patients is under 1500 mg (WHO 2024). The actual intake in Saudi Arabia is 4500 mg daily—three times the limit. Most of this sodium isn't from the salt shaker but from processed products with unexpected salt content:

Potassium: The Unsung Hero in Your Kitchen
Sodium raises blood pressure. Potassium lowers it. This is a simple biological rule: Kidneys use potassium to excrete excess sodium in urine. When potassium is low, sodium stays in the body, and blood pressure rises.
Recommended intake (NHLBI 2024): 3500 - 4700 mg daily. Over 70% of Saudis don't reach half this amount. Here are the best foods from your kitchen to compensate for the deficit:

DASH, Mediterranean, and Modified Saudi Diets
Three diets have proven effective in significantly lowering blood pressure within 6-12 weeks. Each suits a different audience:
DASH
- Fruits & Vegetables: 8-10 servings/day
- Low-fat Dairy: 2 servings
- Whole Grains: 6-8 servings
- Nuts & Legumes: 4-5/week
- Sodium: Under 1500 mg
Mediterranean
- Olive oil as primary fat source
- Fatty fish twice a week
- Nuts & legumes daily
- Limited red meat
- Garlic, lemon, vinegar instead of salt
Modified Saudi
- Kabsa with brown rice + vegetables
- Fattoush salad with olive oil & lemon
- Broth with herbs, not cubes
- Dates instead of sweets
- Reduced salty snacks & pickles
The common principle: more potassium, less sodium, more fiber, unsaturated plant fats. The rest are cultural details.
Medications: When Are They Truly Necessary
Blood pressure medications are among the most disliked by those who take them. Yet, they have saved more lives than any other drug in the past century. The truth is, there are four main classes, each with a different mechanism of action:
ACE Inhibitors
Prevent the formation of a hormone that constricts blood vessels. Arteries relax, and pressure drops. Best for diabetics and those with kidney issues. Common side effect: dry cough (10%).
Angiotensin Receptor Blockers (ARBs)
Work on the same principle as ACE inhibitors but without the cough side effect. A first choice for those sensitive to ACE inhibitors. Protect the kidney in Type 2 Diabetes. Safe and effective for long-term use.
Calcium Channel Blockers (CCBs)
Prevent calcium from entering the muscle cells of arteries, causing them to relax. Best for the elderly and those of African descent. May cause mild ankle swelling.
Diuretics
Flush out sodium and water through urine. Reduce blood volume, thus lowering pressure. A first choice in the AHA 2024 guideline. Cheap and effective. Require potassium monitoring.
• BP Stage 2 (140/90+ mmHg) — Start medication immediately.
• Stage 1 (130-139/80-89 mmHg) with a 10-year cardiovascular risk > 10%.
• Patients with Type 2 Diabetes with BP > 130/80 mmHg.
• Individuals with kidney failure or prior stroke, regardless of BP reading.
When Lifestyle Alone Suffices: Person under 40, no risk factors, with BP in the 'Elevated' range (120-129/<80 mmHg). A 6-month trial of DASH + exercise before considering medication.
Exercise & Sleep: More Potent Than a Pill
Few realize that 30 minutes of daily walking can lower blood pressure as much as a single pill. And an extra hour of sleep per night equals the effect of the entire DASH diet. The body doesn't separate diet, exercise, and sleep—they are all pieces of the same puzzle.
Five Common Myths About Blood Pressure
"I feel my blood pressure when it rises—headache and dizziness."
"Sea salt is healthier than table salt."
"If my BP is normal, I'll stop the medication."
"Young people are safe from high blood pressure."
"One pill is enough for life."
"Licorice is a safe Ramadan drink."
EEINA's 12-Week Blood Pressure Reduction Protocol
Instead of a temporary 'diet,' this is a scientific plan based on DASH, Cochrane, and NICE. Three integrated tiers: daily habits, weekly commitments, and a 12-week outcome. Adhering to all three tiers can clinically lower systolic pressure by 8 to 12 points.
The protocol structure is based on the DASH-Sodium Trial (NEJM 2001), Cochrane Reviews 2023, and Saudi Heart Association 2023 recommendations. Numbers are daily measurable targets.
Habits You Can't Skip
Four numerical targets to practice every day without exception.
Five Tasks to Repeat Weekly
The commitment dose that enhances cumulative effect.
12-Week Checkpoint
A measurable outcome, not just a feeling.
Commitment Rule: Start with one complete tier for two weeks before adding the next. Gradual accumulation builds habit; rushing breaks the plan.
Frequently Asked Questions
-
Measure in the morning before breakfast and medication, and in the evening before dinner. Take two readings a minute apart and calculate the average. Record for two weeks before visiting the doctor. Sit relaxed for 5 minutes before measuring, and do not place the cuff over clothing.
-
Yes, it causes a temporary increase lasting about two hours, which diminishes with regular consumption. Those with uncontrolled high blood pressure should limit their intake to two cups daily and avoid it before measurements and before bedtime. Light Arabic coffee has less impact than espresso.
-
This is White Coat Hypertension, affecting about 25% of people. Clinic anxiety temporarily raises blood pressure. The solution: regular home monitoring for two weeks, or a 24-hour ABPM device for diagnosis. Do not start medication based on a single clinic reading.
-
No. Both are sodium chloride with the same effect on blood pressure. Sea salt contains trace minerals in negligible amounts that make no difference. What matters is the total quantity: under 1500 mg of sodium daily for hypertensive patients. Always read the label.
-
If systolic pressure exceeds 180 or diastolic exceeds 120 with any of the following: chest pain, shortness of breath, blurred vision, sudden severe headache, weakness on one side, or uncontrollable nosebleeds. This is a Hypertensive Crisis requiring urgent intervention. Do not wait—call 997.
-
Never stop on your own. Improved numbers are usually due to the medication itself. Sudden cessation can cause a dangerous rebound, potentially leading to a stroke. Discuss with your doctor after 6 months of a healthy lifestyle to consider gradual dose reduction.
-
Most controlled hypertensive patients can fast safely. Consult your doctor before Ramadan to adjust medication timing (twice daily, at Suhoor and Iftar, instead of morning). Drink 8 cups of water between Iftar and Suhoor. Avoid salty foods and pickles at Iftar. If you feel dizzy or have palpitations, break your fast immediately.
Seven Points to Remember
- Your BP has two numbers. Systolic reflects large artery stiffness, diastolic reflects small artery resistance. Both are important.
- Salt is only 30% of the story. Low potassium, weight, sleep, and stress complete the picture. Don't blame the salt shaker alone.
- Measure at home weekly. Half of Saudi patients are unaware. Measurement is simple, inexpensive, and life-saving.
- The 2:1 rule for balance. Twice the potassium for your sodium intake. A baked potato + dates daily meets half the goal.
- Medication isn't punishment. It's prevention. Sudden cessation kills more than continuous use. Discuss with your doctor, don't decide alone.
- An extra hour of sleep = a full DASH diet. Poor sleep is a major, overlooked cause of hypertension in Saudi Arabia. Sleep apnea is common and hidden.
- Re-measure after 12 weeks of any adjustment to assess actual impact. Numbers don't lie, and feelings can deceive.
Start Your Next Step with EEINA
Smart Meal Plans
Your personalized plan adapts as you progress. Calculated sodium, sufficient potassium.
Get Your Plan →BP-Lowering Recipes
Modified DASH Saudi recipes: Kabsa with brown rice & veggies, Fattoush with pomegranate, Lentil soup with lemon.
Browse Recipes →EEINA App
Daily measurement reminders, BP tracking, and medication alerts. Free.
Download App →


