What is Cholesterol
Cholesterol is a waxy, fat-like substance produced by the liver and used by every cell in your body to build membranes, produce hormones (estrogen, testosterone, cortisol), synthesize Vitamin D, and produce bile acids for digestion. Without it, life is impossible.
Your body produces about 80% of its cholesterol daily. Food contributes only 20%. That is why a "cholesterol-free diet" is a myth—the liver will compensate for any dietary deficit.
LDL and HDL: The Carriers
Cholesterol cannot dissolve in blood. It requires "carriers" (lipoproteins) to travel between the liver and cells. Two main types concern us:
"Bad Cholesterol"
"Good Cholesterol"
The goal is not zero LDL—your body needs some. The goal is balance: low enough LDL to avoid deposition, and high enough HDL to clean what gets deposited.
Triglycerides: The Silent Enemy
Alongside LDL and HDL, the blood contains a third type of fat: Triglycerides. They are the storage form of excess energy in the body. When you eat more sugar or carbohydrates than your body needs, the liver converts them into triglycerides.
Saudi Statistics in Facts
According to the Saudi Heart Association and the Ministry of Health, recent data reveals:
Source: Saudi Heart Association 2023 · MOH Risk Factor Survey 2022 · IDF MENA Atlas 2024.
Seven out of ten Saudis with high cholesterol do not know it, and most are not on treatment. Screening is the first step.
Reading a Lipid Panel: Your Body's Dashboard
When your doctor orders a "lipid panel" (cholesterol test), you receive four numbers. Think of them as a car dashboard, where each gauge has a safe range and a warning range.
Thresholds according to AHA/ACC 2024. Results are guidance, not clinical diagnosis—always consult your physician.
Your Risk Factors: A Self-Assessment
High cholesterol usually causes no direct symptoms. However, risk factors can be actively monitored. Check all that apply to you:
Atherosclerosis: A Lifetime Journey
Atherosclerosis is not a sudden event, but a process spanning decades. It starts early and progresses silently. Here are the four life stages of an artery:
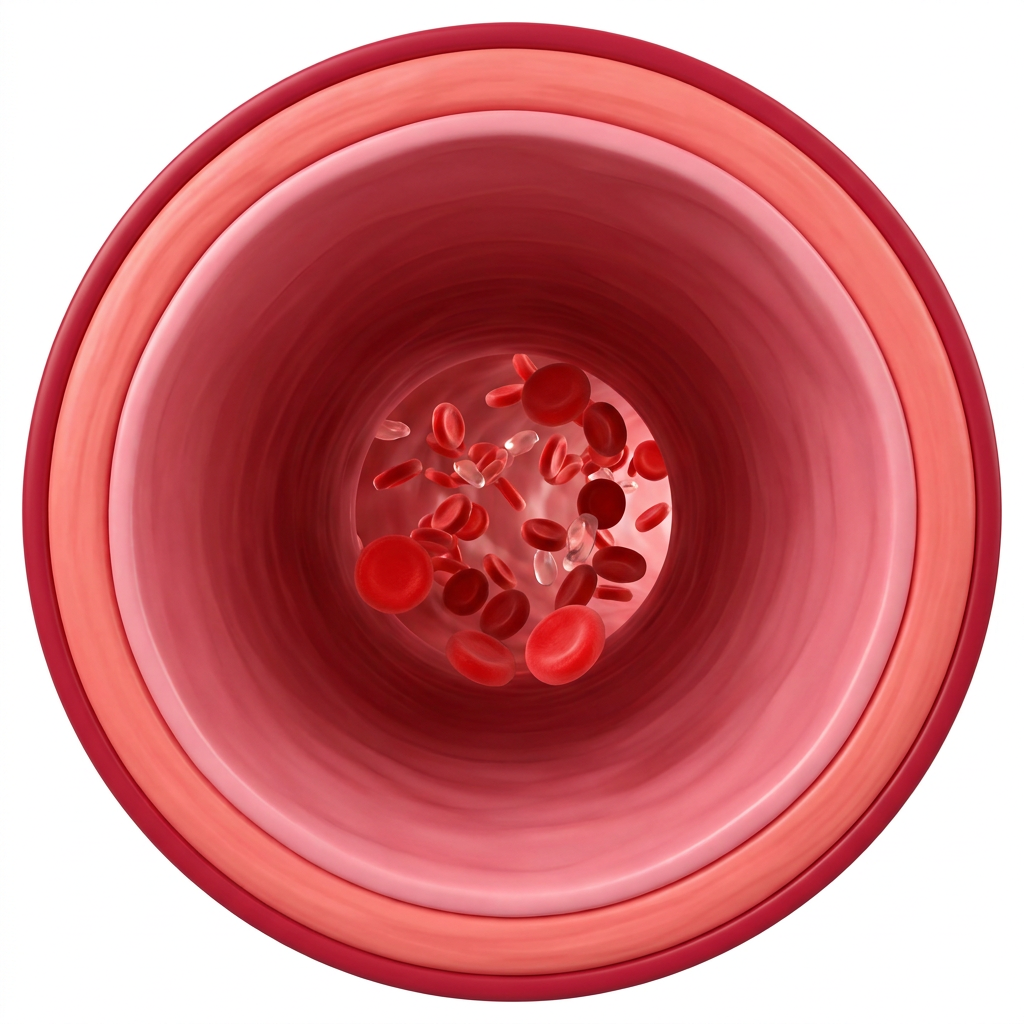
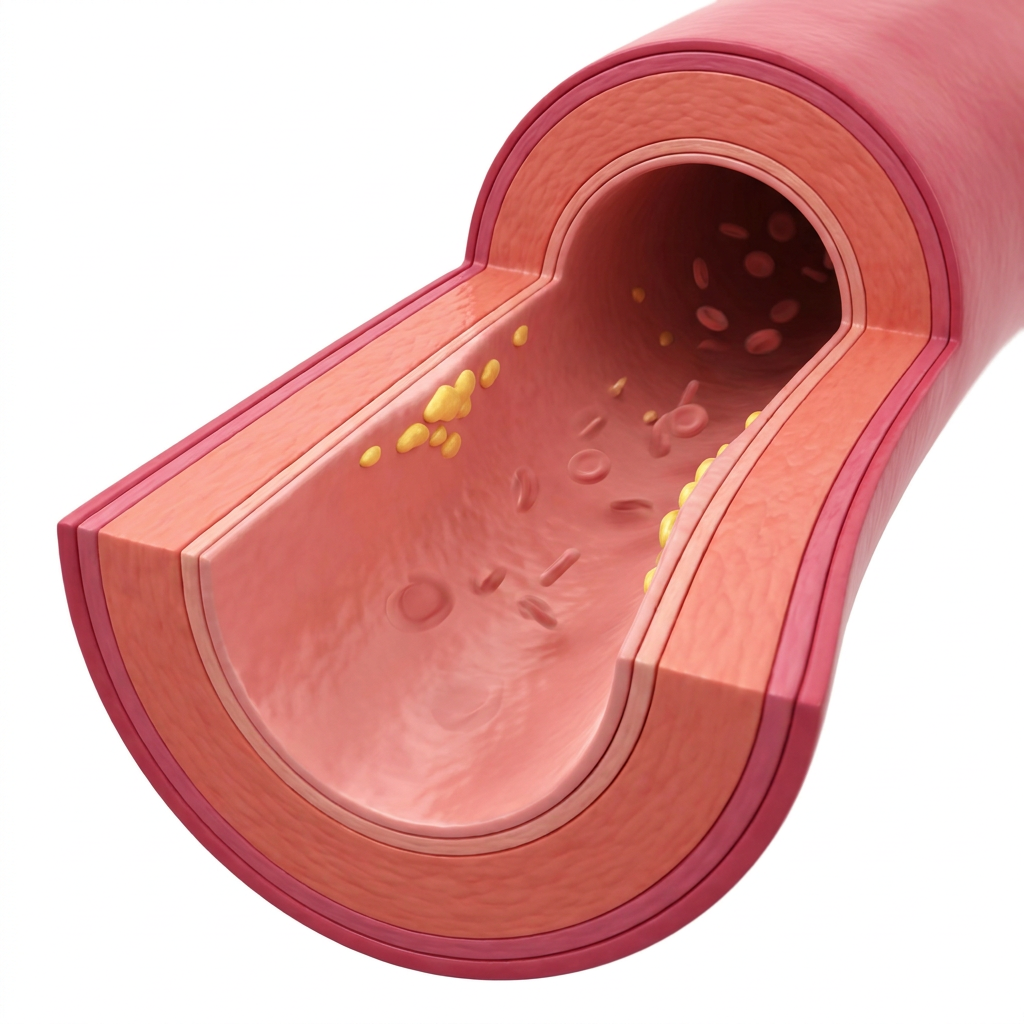
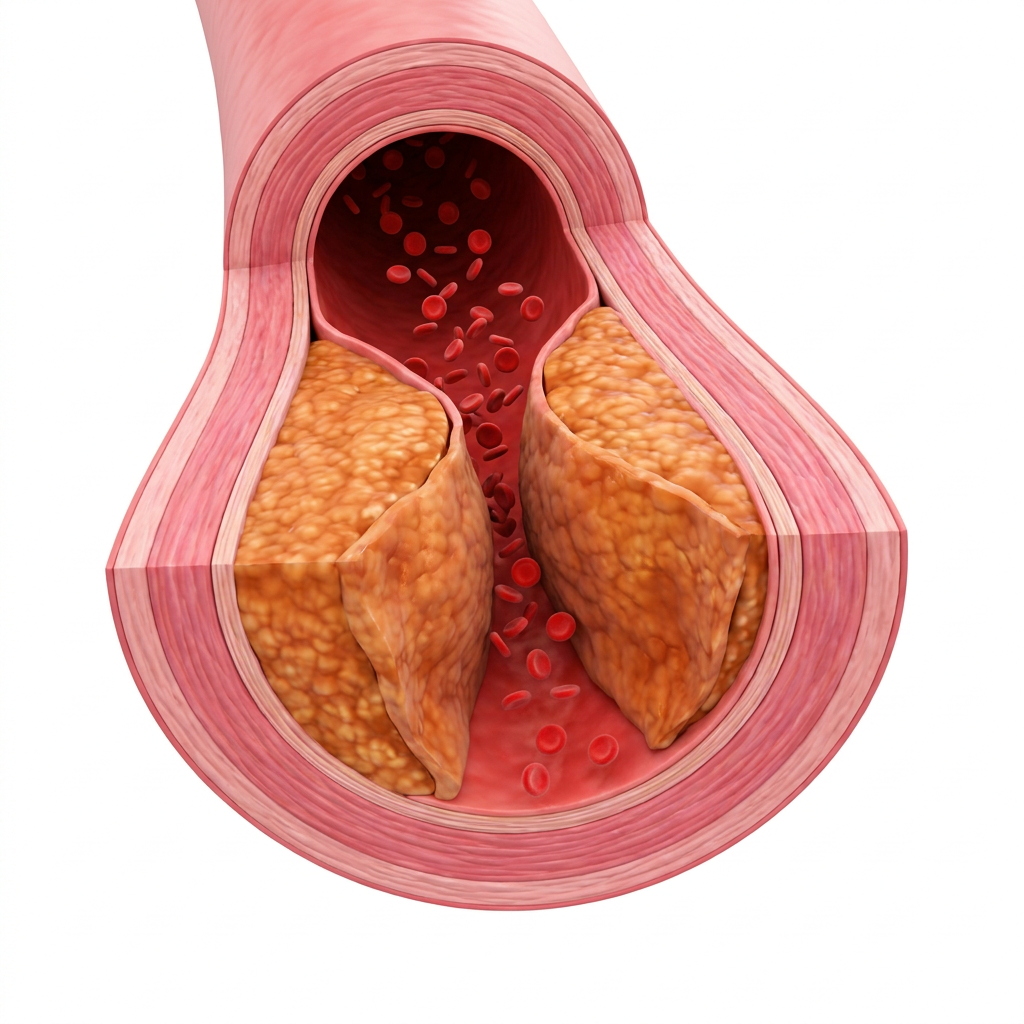
The process started in childhood and progresses silently. Do not wait for symptoms—by the time they appear, the artery is already significantly blocked.
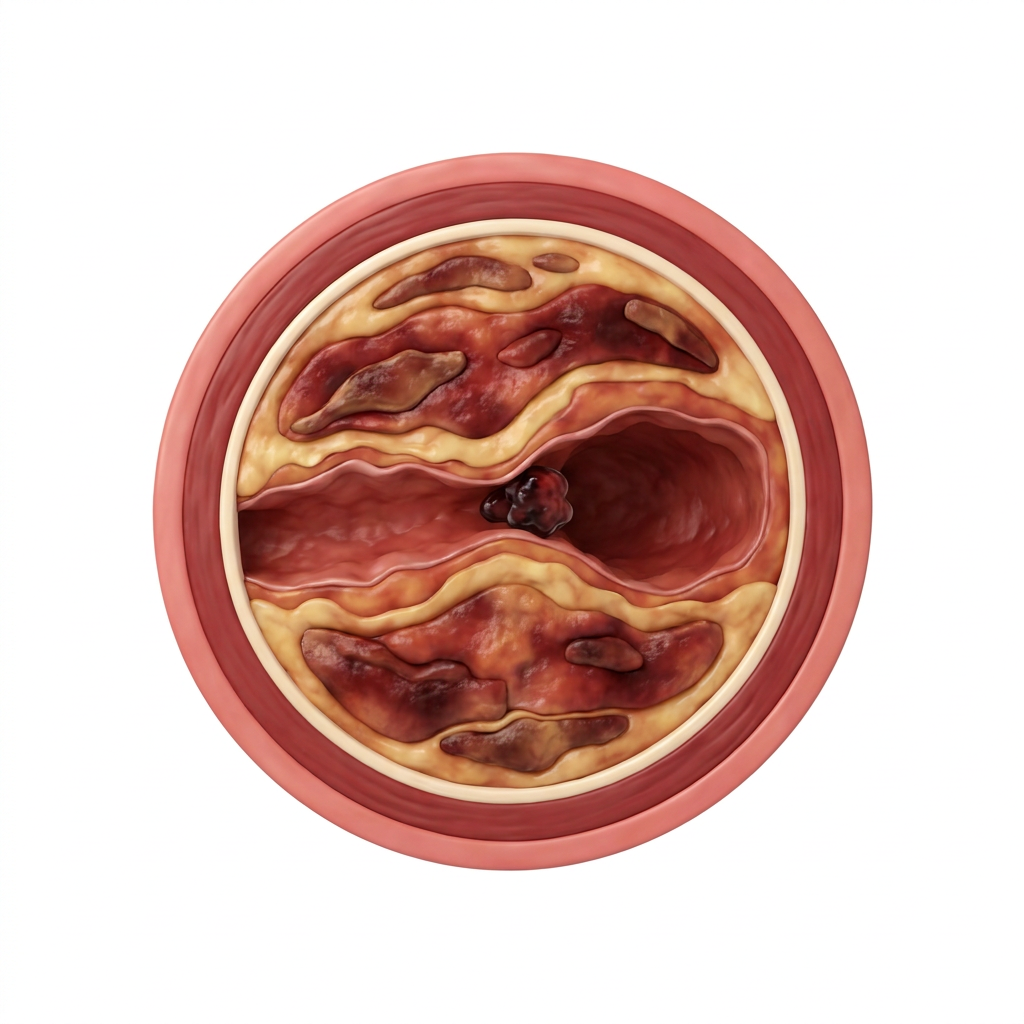
What Happens If Left Untreated
Accumulated plaques do not remain passive. Over time, a plaque may suddenly rupture, causing a blood clot to block the artery. Depending on the location of the blockage, a cardiovascular event occurs:
Heart Attack
Blockage of a coronary artery stops blood flow to heart muscle. Result: death of cardiac tissue within minutes. Every minute of delay worsens damage.
Stroke
Blockage of a cerebral artery. Result can be hemiplegia, loss of speech, or death. Chronic high cholesterol is the leading cause behind 60% of cases.
Peripheral Artery Disease
Atherosclerosis in the leg arteries causes severe muscle pain during walking. In advanced stages, it may necessitate amputation. Highly common alongside diabetes.
Kidney Failure
Cholesterol blocks renal arteries as well. Result: gradual decline in kidney function, which may lead to chronic dialysis.
Seven Foods that Lower Cholesterol
Clinical trials have proven the ability of these foods to lower LDL by measurable percentages within 6 to 12 weeks of consistent consumption. Percentages are averages based on AHA and Cochrane reviews:

Four Foods that Raise Cholesterol
You might be surprised to find that the primary drivers are not eggs or natural butter. The truth:
DASH, Mediterranean, and Modified Saudi Diets
Three diets have proven highly effective in lowering cholesterol, each suited to different audiences:
DASH
- Fruits & Veg: 8-10 servings daily
- Whole Grains: 6-8 servings
- Lean Protein: twice daily
- Nuts: 4-5 times a week
- Sodium: under 2,300 mg
Mediterranean
- Olive oil as primary fat source
- Fatty fish twice a week
- Nuts + legumes daily
- Limited red meat
- Pomegranate or apple cider vinegar
Modified Saudi
- Brown rice Kabsa with vegetables
- Fattoush & pomegranate salads
- Whole-grain brown bread instead of white
- Dates instead of commercial sweets
- Olive oil instead of hydrogenated ghee
The common principle: more fiber, healthy plant-based unsaturated fats, fatty fish, and minimal sugar and trans fats. The rest is cultural detail.
Statins: When Are They Necessary
Statins (Atorvastatin, Rosuvastatin, Simvastatin) are the most effective cardiovascular drugs for lowering LDL and reducing cardiovascular event risk. However, they are not for everyone with elevated cholesterol. Here is how they work:
Without Statins
The liver uses the HMG-CoA reductase enzyme to synthesize cholesterol. Every hour, the liver produces more, particularly at night.
With Statins
Statins block the enzyme. The liver produces less cholesterol, forcing it to pull more LDL from the bloodstream to meet its needs—reducing circulating LDL by 30% to 50%.
• Patients with a prior heart attack or stroke (secondary prevention).
• Patients with LDL above 190 mg/dL (usually genetic).
• Patients with type 2 diabetes and LDL above 70 mg/dL.
• 10-year ASCVD risk exceeding 20%.
When Lifestyle Suffices: Healthy individuals under 40, without multiple risk factors, and LDL under 130 mg/dL.
The New Generation: Beyond Classical Statins
Cholesterol science has progressed rapidly between 2015 and 2024. Four new advancements (unseen in 2005 guidelines) are vital for anyone reading their lab results today:
ApoB — The More Accurate Count
Every atherogenic particle (LDL, VLDL, Lp(a)) carries exactly one ApoB molecule. Measuring ApoB reveals the actual particle count rather than just the cholesterol concentration. Ideal: under 90 mg/dL (general public) or 80 mg/dL (high risk). AHA 2024 recommends it as a superior marker.
Ezetimibe — The Smart Addition
A daily pill that blocks cholesterol absorption in the intestines by 54%. Added to statins, it lowers LDL by an extra 20%. Safe, inexpensive, and widely available as a generic in Saudi Arabia. AHA 2024 advises it before moving to injections.
PCSK9 Inhibitors — The Biologic Generation
Monthly injections (Evolocumab, Alirocumab) lower LDL by 60% beyond statins. Available in Saudi Arabia for patients who do not respond to statins or suffer from muscle pains. Insurance covers qualified cases.
SLCO1B1 — Who Will Experience Pain?
Fewer than 5% of statin users experience actual muscle pain. The SLCO1B1 gene test identifies predisposed individuals before starting treatment. Available in major Saudi labs. The solution is usually switching the drug type or adding CoQ10. Do not stop treatment—ask for an alternative.
Sources: AHA/ACC 2024 Lipid Guidelines · Endocrine Society Statin Intolerance 2023 · Saudi Heart Association Position Paper 2023.
Exercise: How Much Does It Really Lower?
Exercise does not work like a statin, but it is far more powerful than most people think. Meta-analyses (Cochrane 2023) show:
Five Common Myths About Cholesterol
"Eggs raise your cholesterol directly"
"Coconut oil is 100% healthy"
"Coffee always raises cholesterol"
"Statins cause memory loss"
"If you are thin, your cholesterol is safe"
Your Weekly Protocol for Healthy Cholesterol
Instead of a temporary "diet," focus on small habits distributed throughout the week. Adhering to four of these lowers LDL by approximately 15% in 12 weeks:
Retest after 12 weeks to measure the actual impact.
FAQ
-
For most people, eating 1 to 2 eggs daily does not raise blood cholesterol significantly. Dietary cholesterol is different from blood cholesterol. The clinical priority is reducing trans and saturated fats from processed meats, not avoiding whole eggs.
-
Yes. Elevated cholesterol is entirely silent. The AHA and SHA recommend a Lipid Panel screening every 4-6 years starting from age 20, and annually after age 40 or if any risk factors (obesity, diabetes, high blood pressure, family history) are present.
-
6 to 12 weeks of adhering to a heart-healthy dietary pattern (soluble fiber, omega-3, olive oil, and minimal trans fats) lowers LDL by 7% to 15%. Results are faster for those with diet-induced elevation compared to genetic elevation.
-
Often yes, because they address a chronic, ongoing risk factor. However, dosage reduction is highly possible for individuals who radically improve their diet and lose significant weight. Never stop your medication unilaterally—discuss it with your physician after 6 months of strict lifestyle adherence.
-
LDL is a carrier that delivers cholesterol to arteries (excess deposits), while HDL is a carrier that vacuums excess cholesterol from arteries and returns it to the liver for disposal. You want low LDL (under 100) and high HDL (above 60).
-
Unfiltered boiled Arabic coffee contains cafestol and kahweol, which can mildly elevate LDL with heavy daily consumption. Filtered coffees (Drip, V60, Espresso) have no meaningful effect. Moderate consumption (3 small Arabic cups daily) is safe.
-
No. Coconut oil is 82% saturated fat—more than butter. It raises LDL by 5% to 9%. Health claims around it are highly exaggerated. Extra virgin olive oil or avocado oil are far superior clinical choices.
Seven Takeaways to Keep
- Cholesterol is not the enemy. It is vital for every cell. The issue is excess LDL, not cholesterol itself.
- Four numbers, not one. Total, LDL, HDL, and Triglycerides. Each tells a different story.
- Screen before 40. 70% of Saudis do not know their numbers. The test is simple and cheap (Lipid Panel).
- Diet suffices for 70% of cases. 3 servings of oats, walnuts, and salmon weekly lowers LDL by 10%+.
- Statins are not a punishment. They are highly effective prevention for those who need them, lowering LDL by 30% to 50% in weeks.
- Trans fats are the real enemy. Not eggs or natural butter. Always avoid "partially hydrogenated oils" on food labels.
- Retest after 12 weeks of initiating any lifestyle changes to measure actual clinical progress.
Start your next step with EEINA
Smart Meal Plan
Your plan is customized according to your numbers, changing as you progress. Takes your cholesterol into account.
Get Your Plan ←Recipes that Lower LDL
Your modified Saudi recipes: brown rice Kabsa, oatmeal with pomegranate, grilled salmon salad.
Browse Recipes ←EEINA App
Annual screening reminder, track your cholesterol, and walking reminders. Free.
Download App ←


