What is PCOS
PCOS is an abbreviation for Polycystic Ovary Syndrome. It's a chronic hormonal disorder affecting women of reproductive age, resulting in excess androgens (male hormones), irregular ovulation, and the formation of small cysts in the ovaries. However, the term 'cysts' is misleading — these are actually immature egg follicles that haven't been released and accumulate on the ovary's edge.
PCOS is not a single disease, but a syndrome — a collection of symptoms arising from diverse causes. Therefore, it manifests differently in each woman, and treatment must be personalized.
Rotterdam Criteria: How PCOS is Diagnosed
Diagnosis requires the presence of two out of three criteria, according to the Rotterdam consensus 2003, updated in 2023:
1 — Irregular Cycles
Fewer than 8 cycles per year, or more than 35 days between cycles, or complete absence for over 3 months. An indicator of ovulation disorder.
2 — Hyperandrogenism
Signs of excess male hormones: excessive facial or abdominal hair, late-onset acne, male-pattern hair loss on the scalp, or elevated testosterone levels.
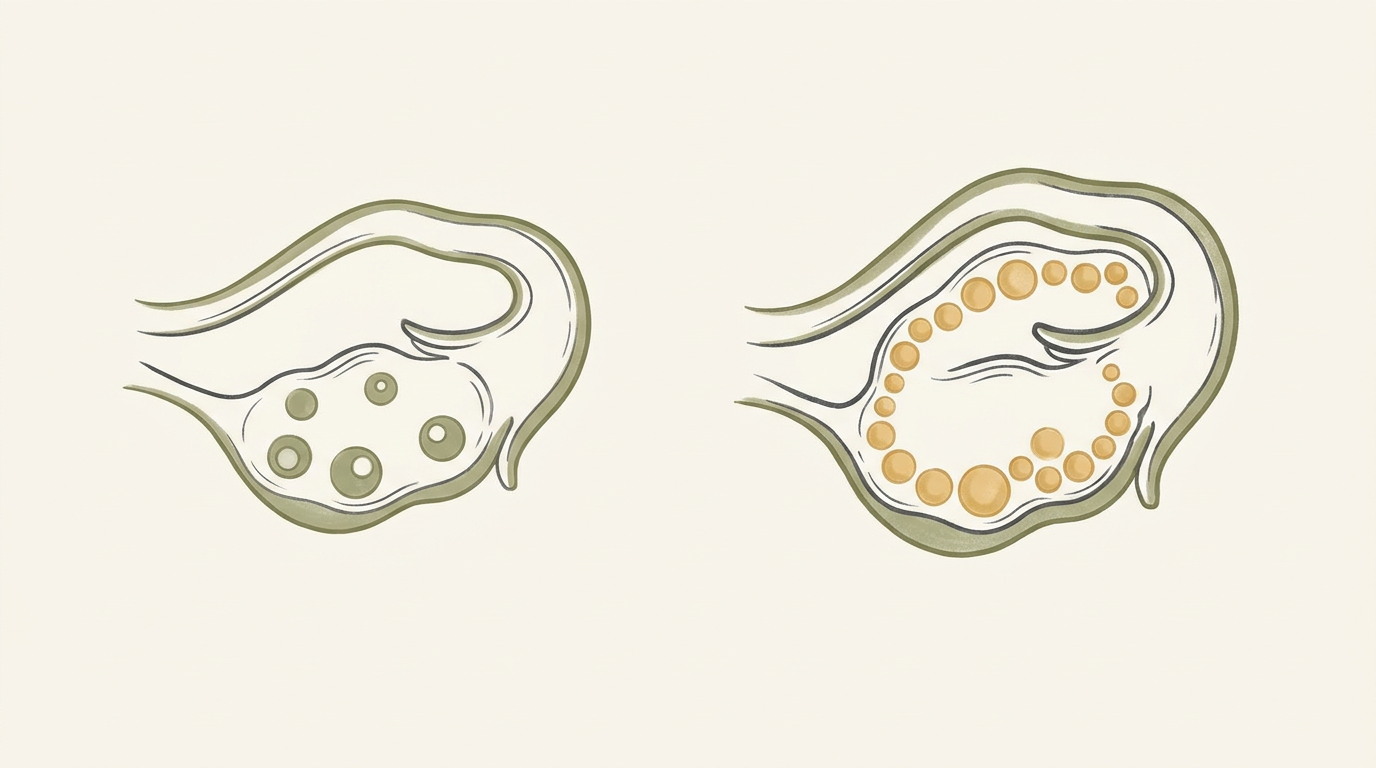
3 — Ovarian Cysts on Ultrasound
The ovary contains 12 or more small follicles (each 2-9 mm), or the ovarian volume exceeds 10 cm³. The characteristic pattern is called 'string of pearls'.
The Four Phenotypes: Which Type Are You?
PCOS has four main phenotypes. Knowing your phenotype helps determine the most suitable treatment:
Classic Phenotype
Irregular Cycle + Hyperandrogenism
Hyperandrogenism + Cysts
Irregular Cycle + Cysts
Two women diagnosed with the same name might have entirely different conditions. PCOS is a spectrum, not a single entity.
Saudi Statistics: The Facts
According to the Saudi Society of Obstetrics and Gynecology and recent studies:
Source: Saudi Society of OBGYN 2023 · KSU Women's Health Study 2024 · ESHRE International Guidelines 2024.
Two out of three women with PCOS in Saudi Arabia do not have an official diagnosis. Many know 'something is wrong' but don't find answers.
Self-Checker — Simplified Rotterdam Criteria
Check the boxes that apply to you. The result is for guidance only, not diagnostic:
Risk Factors That Accelerate PCOS
PCOS is partially genetic, but environmental factors and lifestyle determine its severity. The most significant accelerators are:
Family History
If your mother or sister has PCOS, your chances of developing it are doubled. The genetic predisposition exists even if it doesn't manifest clinically in all family members.
Abdominal Obesity
Fat around the waist secretes enzymes that increase testosterone production. Losing 5% to 10% of body weight can restore menstrual regularity.
Lack of Sleep & Stress
Sleeping less than 7 hours daily raises cortisol and reduces insulin sensitivity. Chronic stress clinically worsens PCOS.
Refined Carbohydrates
Fast-acting carbohydrates raise insulin, and insulin raises androgens. A low-sugar diet improves PCOS with or without weight loss.
Physical Symptoms Your Mirror Tells You
PCOS manifests in various parts of your body. Listen to every signal:
Necessary Tests for Diagnosis
Blood tests + pelvic ultrasound. Request them together from a gynecologist:
The Hidden Root — Insulin Resistance
This is the most crucial section of the article. Seventy percent of women with PCOS have insulin resistance, which is the root cause of most symptoms. High insulin stimulates the ovaries to produce excess testosterone, disrupting ovulation, increasing hair growth, and leading to abdominal fat accumulation.
Treating insulin resistance is the primary clinical treatment for PCOS. The rest are details.
This vicious cycle explains why most traditional treatments (like birth control pills to regulate cycles) don't address the root cause — they only mask symptoms. Improving insulin sensitivity through diet, exercise, metformin, and Inositol addresses the source.
Read the Complete Encyclopedia on Insulin ResistanceSeven Foods That Support Hormone Balance
These foods have demonstrated their ability to clinically improve PCOS symptoms within 12 weeks:

Foods That Increase Inflammation & Insulin
These foods rapidly worsen PCOS. Reducing them is the first step:
Suitable Exercise for PCOS
Not all exercise is equal. Specific types are more beneficial:

Medications, Inositol, & GLP-1
Treatment options range from natural to pharmaceutical:
Myo-Inositol (Natural)
A vitamin-like substance that improves insulin sensitivity and restores ovulation in 70% of cases. Safe during pregnancy. Myo-Inositol with D-Chiro Inositol in a 40:1 ratio is clinically recommended. A first-line option before medication.
Metformin
The traditional first-line option. Improves insulin sensitivity, aids ovulation, and causes slight weight loss. Safe and inexpensive. Side effect: gastrointestinal upset in the first few weeks.
GLP-1 Injections (Ozempic)
Cause 10% to 15% weight loss with significant improvement in PCOS. A strong option for those who haven't succeeded with lifestyle changes. Not used during pregnancy. Expensive and requires a prescription.
Combined Oral Contraceptives (COCPs)
Regulate cycles and reduce excess hair and acne. However, they do not treat the root cause (resistance), only mask symptoms. Useful for those not planning pregnancy currently.
Spironolactone
A medication that blocks androgen receptors on the skin, significantly reducing excess hair and acne within 6 months. Requires contraception (harmful to fetus). A strong option for stubborn hair, but results disappear upon discontinuation.
Letrozole — Ovulation Booster
The global first-line option for stimulating ovulation in PCOS (surpassed Clomid in 2014). Pregnancy rate is 27% per cycle, higher than Clomid's 19%. Lower risk of twins. Requires a prescription from a gynecologist.

PCOS & Pregnancy — Preparing for Motherhood
The most common question women with PCOS ask is: "Will I be able to get pregnant?" The answer is: Yes, in 80% of cases. However, smart preparation makes the difference between years of waiting and joyful motherhood.

Pre-Pregnancy — 3 to 6 Months
Start the lifestyle protocol + Inositol + Vitamin D + 400 mcg folic acid. Check TSH, iron, and HbA1c. Losing 5% of body weight doubles natural pregnancy chances.
When Trying to Conceive
If 6 months of trying pass without conception (with a healthy lifestyle), request ovulation induction with Letrozole. Discuss sperm analysis for your partner in parallel — many cases of delayed conception are treated by addressing both partners.
During Pregnancy
Women with PCOS have double the risk of gestational diabetes and higher preeclampsia rates. Early screening for gestational diabetes (at 12 weeks) is essential. Continuing Inositol is safe and beneficial throughout pregnancy.
Postpartum
Breastfeeding improves insulin sensitivity. However, PCOS does not disappear after childbirth. Take care of yourself as you cared for your baby — returning to your protocol within 3 months protects future pregnancies.
Five Common Myths About PCOS
"PCOS means permanent infertility"
"Surgical removal of cysts cures PCOS"
"Lean women don't get PCOS"
"Birth control pills cure PCOS"
"PCOS is a cosmetic issue, not serious"
EEINA's 12-Week PCOS Balance Protocol
A scientific plan based on ESHRE 2024 and Saudi clinical experience. Three layers. Adherence can restore cycles in 60% of cases.
The protocol is based on ESHRE/ASRM PCOS Guidelines 2024 and Inositol studies in Phytotherapy Research 2022.
Habits to Balance Your Hormones
Four numerical goals each day.
Weekly Balance Commitments
Five tasks to repeat each week.
Measure Progress After 12 Weeks
Measurable results, not just impressions.
The Rule of Return: Losing 5% of body weight restores ovulation in half of cases. You don't need to reach an ideal weight; you need gradual improvement.
Frequently Asked Questions
- Partially. Hormonal symptoms (cycles, hair) subside, but metabolic resistance remains. Postmenopausal women with a history of PCOS have a higher risk of diabetes and heart disease. Lifelong metabolic monitoring is essential.
- Yes, in over 80% of cases. Options range from lifestyle changes + Inositol + Metformin, then Letrozole (global first-line) or Clomid, then ovulation induction injections, and finally IVF. Most women conceive with the first two steps.
- Between 600 and 900 SAR in the private sector. This includes: LH, FSH, Testosterone, DHEA-S, AMH, Fasting Insulin, TSH, and Pelvic Ultrasound. Many labs offer a discounted 'PCOS Package'. It's free in government hospitals.
- Cycles typically improve within 3 to 6 months. Excess hair takes 6 to 12 months. Weight and mood often improve within 4 to 8 weeks. Patience is key — PCOS is not a common cold.
- Yes. Myo-Inositol is a vitamin-like substance safe for years. The recommended dose is 4g daily (2g twice). It's safe during pregnancy and breastfeeding. Available in Saudi pharmacies for 100-180 SAR per month.
- Yes, with conditions. Fasting for 14-16 hours daily can improve insulin sensitivity within 8 weeks. However, lean individuals with Lean PCOS may find it exacerbates their condition. Start with 12 hours and gradually increase, and stop if you notice further cycle disruption.
- The overt hormonal symptoms (cycles, hair, acne) subside with the cessation of ovulation. However, the metabolic root (insulin resistance) persists and becomes more dangerous after menopause. Postmenopausal women with a history of PCOS have double the risk of heart disease and diabetes. Annual metabolic monitoring (HbA1c + blood pressure + cholesterol) is necessary lifelong, even if overt symptoms have subsided.
- There is no clinical evidence for hijama's effectiveness in treating PCOS, but it may help reduce stress if you find the experience relaxing. Honey is a questionable food for PCOS — despite its properties, it's a concentrated sugar that raises insulin. Use it with extreme caution (a small teaspoon per week). Relying on it as a sole treatment misses the opportunity for real treatment.
- If their cycle is irregular 2 years after starting menstruation, or if they have severe acne + excess hair + weight gain, seek an evaluation from a gynecologist specializing in adolescents. Early diagnosis can prevent years of delay.
Seven Points to Take With You
- PCOS is a hormonal metabolic disorder, not a cyst disease. The root is insulin resistance in 70% of cases.
- The two-out-of-three rule. Rotterdam criteria require two of: irregular cycle + hyperandrogenism + cysts.
- Four phenotypes, not one. Knowing your phenotype determines the most suitable treatment.
- Request fasting insulin + HOMA-IR. The most important test to reveal the root cause.
- Two cups of spearmint tea daily. The simplest natural treatment for hyperandrogenism.
- Resistance training is strongest. More effective than cardio for PCOS clinically.
- Inositol first, then Metformin. A safe natural option before medication.



